







Sex After Birth: When It’s Safe After Childbirth, Why It Hurts, and What Helps Pain, Dryness, Low Libido & Vaginal Laxity
Six months after giving birth, a lot of women are still waiting for things to feel normal again. Most are told to be patient. Fewer are told that patience is not always the right medical advice.

MEDICALLY REVIEWED BY
Op. Dr. Arzu Bebek
Gynecologist & Women’s Sexual Health Specialist – Dr. Terziler Exclusive Clinic, Istanbul
Last updated: May 2026
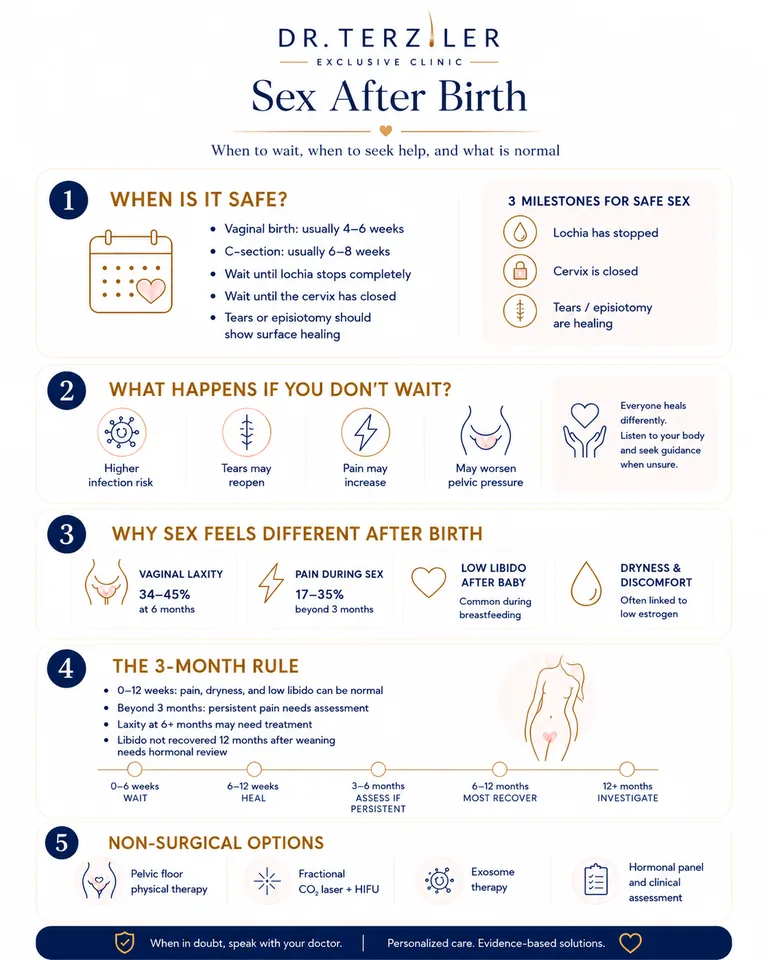
Most doctors advise waiting 4–6 weeks after birth before having sex. Pain, dryness, and changed sensation in the first 6–12 weeks are common. When symptoms persist beyond 3 months (particularly dyspareunia, vaginal laxity, or lost libido) they may indicate conditions that require clinical assessment, not more waiting.
When Can You Have Sex After Childbirth
The standard clinical recommendation is to wait 4–6 weeks after vaginal delivery and 6–8 weeks after C-section before resuming sex. This timeline is based on ACOG and NHS guidance: it allows the cervix to close, lochia to stop, and acute tissue trauma to heal (American College of Obstetricians and Gynecologists, Committee Opinion No. 736, 2018; NHS, nhs.uk/pregnancy).
Three milestones must be reached before sex is physically safe for women’s sexual health:
Lochia (postpartum uterine discharge) stops completely; typically at 4–6 weeks
The cervix closes; this occurs in parallel with lochia cessation
Any episiotomy or perineal tear shows surface healing; internal healing continues for weeks beyond this
Vaginal delivery vs C-section. After vaginal delivery, recovery centres on the perineum, pelvic floor, and vaginal mucosa. After C-section, the abdominal and uterine incisions need structural integrity; but hormonal changes still affect vaginal mucosa regardless of delivery route.
What Happens If You Don’t Wait 6 Weeks after Birth?
Having sex before lochia stops carries a clear and specific infection risk. While the cervix remains partially open, bacteria from the vaginal canal can ascend into the uterine cavity; increasing the risk of endometritis and pelvic inflammatory disease. Unhealed perineal tears can reopen under friction. In women with connective tissue vulnerability, early resumption can worsen underlying pelvic organ descent (ACOG Practice Bulletin, 2018).
The risk is proportional to timing: sex before 3 weeks is significantly higher risk than sex at 5 weeks. Sex before 6 weeks postpartum is not a uniform prohibition; it is a threshold based on biological markers, not a calendar date. The safest rule: wait until lochia stops, confirmed tears are closed, and discomfort is absent.
Not sure if it is safe yet?
Send your symptoms and delivery type. The clinical team can tell you whether you need more healing time or an assessment.
Why Sex Feels Different After Birth and When That Is Not Normal
Sex feels different after birth for most women. Physiological changes (reduced estrogen, altered pelvic anatomy, pelvic floor muscle change) are near-universal in the early postpartum period. What varies is severity and whether symptoms resolve on their own. Symptoms that improve steadily are normal healing. Symptoms that plateau or worsen after 3 months require clinical evaluation.
Vaginal Laxity: Does Sex Feel Loose After Birth
Vaginal laxity after childbirth is reported by 34–45% of women at 6 months postpartum, resulting from stretching of pelvic floor muscles and fascial support structures during delivery.
During vaginal delivery, the pelvic floor muscles, fascial supports, and levator ani complex stretch significantly; sometimes tearing. The vaginal canal can remain wider than pre-pregnancy for months. Most articles on postpartum sex frame this as a muscle weakness problem solved by Kegel exercises.
This is only half the picture. Kegel training strengthens pelvic floor muscles. It does not restore fascial integrity. When the connective tissue layer anchoring the vaginal walls loses tensile strength, this is structural fascial laxity; a separate issue requiring tissue-level treatment, not muscle rehabilitation alone.
Source: Bø K et al., Neurourol Urodyn. 2017;36(2):221–244. PMID: 27918661
Postpartum Dyspareunia: When Pain Is Not Just Soreness
Postpartum dyspareunia persisting beyond 3 months affects 17–35% of women and is not resolved by waiting alone when the underlying cause is estrogen-deficiency vaginal atrophy or scar tissue formation. (Buhling KJ et al., ‘Rate and risk factors of dyspareunia after delivery,’ Arch Gynecol Obstet. 2006;274(1):17–24. PMID: 16450103).
The causes fall into four distinct categories are shown below.
Scar tissue formation
Inelastic remodelling at episiotomy or tear repair sites creates a rigid band that causes sharp, localised pain on penetration
Genitourinary Syndrome of the Postpartum Period
Prolonged breastfeeding suppresses estrogen production, causing vaginal mucosal thinning, reduced lubrication, elevated vaginal pH, and increased tissue fragility; an identical pathophysiology to GSM in menopause, but occurring in women in their 20s and 30s post-birth. Most postpartum content does not name or explain this condition.
Pelvic floor hypertonia
A paradoxical state where the pelvic floor muscles are overly contracted, not weak. This creates painful muscular resistance during penetration. It is the opposite of laxity and is treated differently; physiotherapy, not energy devices.
Endometriosis activation
Postpartum hormonal fluctuations can reactivate previously quiescent endometriosis lesions in genetically predisposed women
Source: Buhling KJ et al., Arch Gynecol Obstet. 2006;274(1):17–24. PMID: 16450103
Lost Libido After Baby: How Long Is Normal
Prolactin secretion during breastfeeding suppresses estrogen and testosterone, reducing libido by a clinically significant degree; a physiological effect that reverses within 3–6 months of weaning in most women.
Prolactin (produced during breastfeeding) directly suppresses estrogen and testosterone. Testosterone levels drop 40–50% in the first 6 months postpartum (Alder EM et al., Br J Psychiatry. 1986;148(1):74–79. PMID: 3697573). Low or absent libido throughout the breastfeeding period is a predictable physiological response, not a relationship or psychological problem.
The clinical threshold: libido that has not recovered 12 months after stopping breastfeeding is not normal postpartum adjustment. No sex drive after baby 24 months signals a persistent hormonal or metabolic issue, not ongoing adaptation.
For women whose libido remains low beyond 12 months after weaning, the Youngevity™ Reset Programme includes a full hormonal panel: testosterone, estradiol, SHBG, DHEA-S; plus genetic analysis examining over 750,000 to 3.000.000 variants linked to endocrine function and metabolic health. The programme produces a clinical explanation and personalised protocol, not a generic reassurance. This is part of a broader longevity and Youngevity approach that treats the postpartum body as a system, not a series of isolated symptoms.
Hormones still feel off after birth?
Ask about the Youngevity Reset hormonal panel for postpartum recovery.
What Is the 3-Month Rule after Birth? When to Stop Waiting and Seek Help
The 3-month rule is a clinical threshold, not a cultural waiting period. Before 3 months postpartum, most sexual symptoms (pain, dryness, reduced sensation, low libido) fall within the range of expected healing. After 3 months, persistent symptoms indicate an underlying condition that requires targeted treatment, not continued waiting.
Wait it out: normal postpartum adjustment:
- Pain or discomfort during sex in the first 6–12 weeks, particularly in areas of surface healing
- Vaginal dryness and reduced lubrication during active breastfeeding
- Reduced or absent libido throughout the breastfeeding period
- Mild pelvic pressure or heaviness that decreases with rest
- Occasional light spotting on first resumption at 6 weeks
Seek clinical assessment: beyond normal adjustment:
- Dyspareunia (pain during sex) persisting or worsening beyond 3 months postpartum
- Vaginal laxity causing significant sensation change at 6+ months
- Libido not recovering 12 months after stopping breastfeeding
- Stress urinary incontinence (leaking when coughing, sneezing, or jumping) beyond 3 months
- Visible or palpable perineal scar tissue causing sharp localised pain or altered sensation
Still unsure where your symptoms fit?
Tell us what changed, when it started, and whether you are breastfeeding. We will guide the next step confidentially.
What Are the Non-Surgical Treatments for Postpartum Vaginal and Sexual Function?
When structural or hormonal postpartum changes persist beyond the natural recovery window, clinical intervention accelerates tissue repair. The following are evidence-based non-surgical options available at Dr. Terziler Exclusive Clinic. Each is a medical treatment when the clinical indication is functional impairment.
Fractional CO2 Laser and HIFU: Tissue Regeneration
Fractional CO2 laser delivers calibrated thermal energy to the vaginal mucosa in a pixelated micro-ablative pattern. This stimulates rapid local collagen remodelling, increases mucosal thickness, normalises vaginal pH, and restores lubrication. Controlled studies report improvement across all four parameters at 3 months post-treatment, with results sustained at 12-month follow-up (Zerbinati N et al., ‘Microscopic and ultrastructural modifications of postmenopausal atrophic vaginal mucosa after fractional CO2 laser treatment,’ Lasers Med Sci. 2015;30(1):429–436. PMID: 25395284).
Read more
For deeper fascial laxity in laser vaginal rejuvenation (where the structural connective tissue layer beneath the mucosa needs remodelling) HIFU (High-Intensity Focused Ultrasound) targets tissue depths inaccessible to surface energy devices. HIFU stimulates structural collagen synthesis at the fascial layer, addressing the component of laxity that Kegel exercises cannot reach.
Morpheus8 Body + RF Microneedling: Pelvic Floor Structural Support
Morpheus8 delivers bipolar radiofrequency energy through microneedles into subdermal tissue layers. In postpartum patients, the primary indication is perineal and labia majora remodelling; stimulating collagen synthesis in stretched fascial tissue that standard energy devices do not reach. RF energy at this depth drives a measurable increase in local collagen density within 8–12 weeks of treatment. The mechanism is thermal remodelling of dermal and subdermal collagen architecture, producing structural tightening without surgical intervention.
Exosome Therapy: Mucosal and Nerve Regeneration
Exosomes derived from mesenchymal stem cells (MSCs) deliver paracrine signalling molecules that promote mucosal regeneration, neo-vascularisation, and nerve repair at the cellular level (Rani S & Ritter T, Adv Mater. 2016;28(27):5542–5552. PMID: 27100153). In postpartum patients, the primary clinical indications are:
Read more
- Persistent mucosal thinning unresponsive to topical estrogen or lubricants
- Nerve hypersensitivity or allodynia from perineal trauma during delivery
- Scar tissue remodelling at episiotomy or deep tear sites
- Reduced mucosal vascularisation contributing to chronic dryness
Pelvic Floor Physical Therapy (First-Line for Hypertonia)
For pelvic floor hypertonia (where muscles are too contracted, not too weak) energy-based treatments are contraindicated as a first step. Physiotherapy with internal manual release and neuromuscular re-education is the first-line clinical recommendation before any device-based intervention (Bø K et al., Neurourol Urodyn. 2017;36(2):221–244. PMID: 27918661). Proceeding directly to a laser or RF device in a patient with undiagnosed hypertonia worsens pain.
Which non-surgical option fits your symptoms?
Ask whether your pattern sounds like dryness, laxity, scar pain, hypertonia, or hormones before choosing treatment.
What to Expect After Birth: A Week-by-Week Recovery and Sex Timeline
Every postpartum recovery differs. The table below reflects general clinical thresholds, not a guarantee that symptoms resolve at each stage. Use it as a decision framework, not a fixed schedule.
| Timeline | What Is Normal | When to Act |
|---|---|---|
| 0–6 weeks | Pain, dryness, spotting on resumption. Lochia present. | Do not resume sex until lochia stops completely. |
| 6–12 weeks | Discomfort, low libido, mild dryness during breastfeeding. | Lubricant. Pelvic floor rehab. No procedural intervention yet. |
| 3–6 months | Most women recovered. Some residual pain or laxity. | If pain persists beyond 3 months → clinical assessment. |
| 6–12 months | Full recovery expected in most cases. | Persistent laxity or pain → consider non-surgical treatment. |
| 12–18 months | Libido recovering after breastfeeding ends. | Low libido at 18 months → hormonal panel + assessment. |
| 18+ months | Symptoms at this stage are no longer postpartum. | Independent gynaecological condition. Investigate separately. |
What Is Vaginal Rejuvenation After Childbirth?
Non-surgical vaginal rejuvenation with fractional CO2 laser and HIFU is classified by the EAU and ISAPS as a functional treatment when the indication is postpartum GSM or pelvic floor laxity, not an aesthetic procedure.
Vaginal rejuvenation is widely perceived as a cosmetic procedure. In the postpartum context, this framing is clinically inaccurate. When the indication is postpartum dyspareunia, Genitourinary Syndrome of the Postpartum Period (GSPP), or pelvic floor fascial laxity causing measurable functional impairment, non-surgical intervention qualifies as medical treatment.
This distinction matters practically. Women in the UK, Australia, and Canada who are navigating NHS or insurance pathways need to know whether their condition qualifies as functional (and therefore potentially covered) or cosmetic. It also matters for women who would reject vaginal cosmetic surgery but would readily accept a functional medical treatment addressing a documented clinical condition. Those are the same procedure. The clinical indication determines the category, not the anatomical location.
Source: EAU Guidelines on Female Pelvic Floor Disorders, uroweb.org, 2023 | ISAPS Global Statistics, isaps.org, 2023
What About Aesthetic Concerns After Birth
Childbirth changes the external appearance of the perineal area for many women: labial asymmetry with Barbie Aesthetics, stretched tissue, and altered contour are common findings. These changes are distinct from functional complaints like pain, laxity, or incontinence; but they affect body image and confidence in a way that is clinically significant. Non-surgical tissue remodelling and labiaplasty address these concerns safely when performed by a trained specialist.
Want to understand your postpartum treatment options?
Book a confidential consultation for functional concerns, aesthetic changes, or both.
Why Choose Istanbul for Postpartum Sexual Health Treatment
Women in the UK, US, and Australia typically encounter two obstacles: NHS or insurance waitlists of 6–18 months for pelvic specialists, and private clinics that classify vaginal rejuvenation as cosmetic rather than clinical, pricing it accordingly. Istanbul has become a serious alternative precisely because neither obstacle applies.
Postpartum sexual health treatments at Dr. Terziler Exclusive Clinic run 55–70% less than equivalent private care in Western Europe or North America. Wait times are measured in days. A comprehensive postpartum assessment and treatment plan can be completed in a 3–4 day visit.
Dr. Terziler Exclusive Clinic differentiates on clinical standard, not price alone:
AAACI accreditation
Internationally recognised safety and clinical protocol standard, equivalent to Western European benchmarks, rare among Turkish clinics
Diagnosis before treatment
Every postpartum patient receives a hormonal panel, pelvic floor evaluation, and tissue assessment before any procedure is recommended
Led by Dr. Arzu Bebek
Dr. Arzu Bebek leads the gynaecological and postpartum sexual health programme, with specialist training in functional and aesthetic intimate health
Youngevity Reset integration
For patients whose postpartum symptoms extend into hormonal imbalance, the Longevity (Youngevity™ Reset programme) provides a full endocrine and genomic workup (analysing up to 3,000,000 genetic variants) to address the root cause, not the surface symptom
Planning treatment in Istanbul?
Share your timeline and symptoms. Our team will explain what can be assessed in a 3-4 day visit.
Frequently Asked Questions
Most clinical guidelines recommend waiting 4–6 weeks after vaginal delivery and 6–8 weeks after C-section. The minimum biological requirement is that lochia stops completely and any episiotomy or perineal tear shows surface closure. These are the physical markers of readiness — the calendar date is secondary. (ACOG Committee Opinion No. 736, 2018; NHS, nhs.uk)
Vaginal laxity after childbirth is reported by 34–45% of women at 6 months postpartum. It results from stretching of the pelvic floor muscles, vaginal walls, and fascial support structures. Kegel exercises strengthen muscle tone but do not restore structural fascial integrity. Laxity that persists beyond 6 months and causes significant sensation change warrants clinical assessment. Non-surgical options (CO2 laser, HIFU) address both muscular and fascial components.
Persistent dyspareunia beyond 3 months affects 17–35% of postpartum women (Buhling KJ et al., Arch Gynecol Obstet. 2006). Common causes: estrogen-deficiency vaginal atrophy (Genitourinary Syndrome of the Postpartum Period), scar tissue at episiotomy or tear sites, pelvic floor hypertonia (muscles too tight, not too loose), and postpartum endometriosis activation. None of these resolve with waiting alone. Each requires a specific treatment pathway.
Before lochia stops and the cervix closes (typically 4–6 weeks) bacteria can ascend from the vaginal canal into the uterine cavity, increasing the risk of endometritis and pelvic inflammatory disease. Unhealed perineal tears can reopen under friction. For C-section patients, the uterine incision integrity is an additional consideration. Sex at 3–4 weeks postpartum carries a significantly elevated infection risk compared to sex at 5–6 weeks.
Prolactin suppresses estrogen and testosterone throughout breastfeeding. Testosterone drops 40–50% in the first 6 months postpartum. For breastfeeding women, low or absent libido is a normal physiological state. After weaning, libido typically recovers within 3–6 months. Libido that has not recovered 12 months after stopping breastfeeding (including ‘no sex drive after baby 24 months’) is a clinical finding requiring hormonal assessment.
Yes, when indicated for postpartum dyspareunia, vaginal laxity, or Genitourinary Syndrome of the Postpartum Period, vaginal rejuvenation is a medical intervention, not an aesthetic choice. Non-surgical options including fractional CO2 laser, HIFU, and exosome therapy address tissue thinning, structural laxity, and mucosal damage at the cellular level. Treatment must follow proper clinical assessment, including pelvic floor evaluation to rule out hypertonia before device-based treatment begins.
No. At 3–4 weeks postpartum, lochia is still present in most women and the cervix has not fully closed. This window carries an elevated infection risk, the partially open cervix creates a direct pathway for ascending bacteria. Some women feel physically healed by 4 weeks, particularly after straightforward vaginal deliveries without tears. Physical comfort does not equal biological safety at this stage.
Sources
All clinical claims in this article are supported by peer-reviewed literature or authoritative clinical guidelines. Full references are listed below.
Clinical guidelines
- 1. ACOG Committee Opinion No. 736. Optimizing Postpartum Care. American College of Obstetricians and Gynecologists. 2018.
- 2. NHS. Sex and contraception after birth. nhs.uk.
- 11. EAU. EAU Guidelines on Female Pelvic Floor Disorders. European Association of Urology. 2023.
- 12. IUGA. International Urogynecological Association. Female Pelvic Floor Disorders Guidelines.
Postpartum symptoms and pelvic floor
- 3. Buhling KJ et al. Rate and risk factors of dyspareunia after delivery. Arch Gynecol Obstet. 2006;274(1):17–24.
- 4. Alder EM et al. Hormones, mood, and sexuality in lactating women. Br J Psychiatry. 1986;148(1):74–79.
- 5. Bø K et al. IUGA/ICS joint report on terminology for conservative management of female pelvic floor dysfunction. Neurourol Urodyn. 2017;36(2):221–244.
- 6. Hutchinson-Colas J & Segal S. Genitourinary syndrome of menopause and the use of laser therapy. Maturitas. 2015;82(4):342–345.
Regenerative and device evidence
- 7. Zerbinati N et al. Microscopic and ultrastructural modifications of postmenopausal atrophic vaginal mucosa after fractional CO2 laser treatment. Lasers Med Sci. 2015;30(1):429–436.
- 8. Rani S & Ritter T. The Exosome — A Naturally Secreted Nanoparticle and its Application to Wound Healing. Adv Mater. 2016;28(27):5542–52.
- 9. Alster TS & Tanzi EL. Noninvasive lifting of arm, thigh, and knee skin with transcutaneous intense focused ultrasound. Dermatol Surg. 2012;38(5):754–759.
- 10. ISAPS. Global Statistics: International Survey on Aesthetic/Cosmetic Procedures. isaps.org, 2023.
Located in Istanbul, Turkey, Dr. Terziler Exclusive Clinic provides women’s sexual health, postpartum recovery, longevity, regenerative medicine, and medical aesthetics care through specialist-led, confidential clinical pathways for international patients.